ARTICLE
Clinical Psychology and Perinatal Mental Health Programs in hospitals in the Community of Madrid: Description and recommendations of Good Practices
Programas de Psicología Clínica y Salud Mental Perinatal en Hospitales la Comunidad de Madrid: Descripción y Recomendaciones de Buenas Prácticas
 Isabel Cuellar-Flores icuellarflores@gmail.com
Laura Alvarez-Cienfuegos Cercas
Sara Arias Rubio
Elena Cordero
Mónica Díaz de Neira
Arantxa Fernández
Elena Lanza Raggiotti
María Serrano-Villar
Ana Madrigal
Ana Hernanz Vaquero
Lorena Velayos Jiménez
Belén Eimil Ortiz
Laura Pérez
Mónica Jiménez
Carlos Jordán
María Dieguez Porres
Isabel Cuellar-Flores icuellarflores@gmail.com
Laura Alvarez-Cienfuegos Cercas
Sara Arias Rubio
Elena Cordero
Mónica Díaz de Neira
Arantxa Fernández
Elena Lanza Raggiotti
María Serrano-Villar
Ana Madrigal
Ana Hernanz Vaquero
Lorena Velayos Jiménez
Belén Eimil Ortiz
Laura Pérez
Mónica Jiménez
Carlos Jordán
María Dieguez Porres
Clinical Psychology and Perinatal Mental Health Programs in hospitals in the Community of Madrid: Description and recommendations of Good Practices
Papeles del Psicólogo, vol. 45, no. 2, pp. 108-115, 2024
Consejo General de Colegios Oficiales de Psicólogos
Received: 28 July 2023
Accepted: 05 October 2023
Abstract: Specific attention to perinatal mental health is a key element in the healthcare system. In Spain and in the Community of Madrid, concern for perinatal mental health has been increasing in recent years. The objective of this work is to identify and describe the main perinatal psychological care programs and the first thousand days in the hospitals of the Madrid Health Service. Twelve Hospitals with complete or partial programs were identified. Their organizational and care characteristics are described. The ratios of perinatal clinical psychologists range from 0.04 to 0.51/10,000 deliveries and from 0.08 to 0.78/20 neonatology cribs in the region. Perinatal mental health care programs in the Madrid hospital network have been consolidated and expanded; however, there are inequities in the availability of this care. Good practice recommendations for implementing and improving these programs are provided.
Keywords: Perinatal psychology, Perinatal mental health, Perinatal grief, Good practices.
Resumen: La atención específica a la salud mental perinatal es un elemento clave en el sistema sanitario. En España y en la Comunidad de Madrid la preocupación por la salud mental perinatal ha venido incrementándose en los últimos años. El objetivo de este trabajo ha sido identificar y describir los principales programas de atención psicológica perinatal y a los primeros mil días de vida en los hospitales del Servicio Madrileño de Salud. Se han identificado doce hospitales con programas completos o parciales de los que se describen sus características organizativas y asistenciales. Las ratios de psicólogos/as clínicos/as perinatales van de 0.04 a 0.51/10000 partos y de 0.08 a 0.78/20 cunas de neonatología en la región. Los programas de atención a la salud mental perinatal en la red de hospitales madrileños se han consolidado y expandido, sin embargo existen inequidades en la disponibilidad de esta atención. Se proporcionan recomendaciones de buenas prácticas para implementar y mejorar estos programas.
Palabras clave: Psicología perinatal, Salud mental perinatal, Duelo perinatal, Buenas prácticas.
Introduction
Specific attention to perinatal mental health is a key element for better clinical outcomes in pregnancy, childbirth, and early infant life (World Health Organization -WHO, 2022). In addition to prevention and screening measures, the World Health Organization (WHO) recommends early mental health intervention from maternal and child services, integrating this type of care effectively into existing services, and providing phased, inclusive, person-centered care (WHO, 2022).
The paradigm of care for the first 1,000 days (Conecta Perinatal, 2023; p. 128) complements or extends perinatal mental health care to the first two years of a child's life. These programs have been adopted in several countries in Latin America and Europe with the objective of improving well-being, including the emotional well-being, of mothers, fathers, siblings, and infants, and their implementation has recently been announced in some hospitals in Madrid (Tragacete, 30 March 2023).
These recommendations are based on the high prevalence of mental disorders and emotional distress during this period. One in 10 mothers in high-income countries will experience a mental health problem during pregnancy or in the year after delivery (WHO, 2022). Specifically in Spain, about 15% of women in the prenatal period and 27% in the postnatal period (Besteiro et al., 2001; Rodríguez-Muñoz et al., 2023) experience perinatal depression. Furthermore, having a newborn child in neonatology constitutes a risk situation for presenting mental disorders during the baby's first year of life (Hynan et al., 2013), and people who lose a child during the perinatal period are at high risk of presenting a psychological disorder (Burden et al. 2016). Another specific area is assisted reproduction, which can involve high emotional stress (Burgio et al., 2022).
It is known that postpartum depression is currently underdiagnosed (WHO, 2022), and very little attention is given to the perinatal emotional distress of the father. There is also evidence that stress and emotional distress during pregnancy is associated with an increased likelihood of preterm birth (Staneva et al., 2015), and with children presenting mental health problems and lower intellectual capacity (Bauer et al., 2015).
Therefore, numerous guidelines emphasize that the assessment, detection, and intervention of mental health problems during pregnancy and the postpartum period are essential to ensure the physical and emotional well-being of the mother, father, and baby (National Institute for Health and Care Excellence-NICE, 2018) and recommend actively assessing them (Austin et al., 2017; NICE, 2018). In addition, intervening on them can be cost-effective (Bauer et al., 2014).
The World Health Organization (WHO, 2022) states that this care should be provided by psychologists trained in this field, in the context of maternal and child services, in the case of mild-moderate problems, and in the specialized mental health setting for moderate-severe problems. However, it is estimated that about 85% of women with depression during the perinatal period are not adequately treated (Goodman & Tyer-Viola, 2010). For this reason, expert groups have made recommendations on the number of professionals that would be necessary to ensure the accessibility of psychological treatments. In the United Kingdom, it has been recommended that there should be one full-time clinical psychologist for every 20 neonatal care beds (Atkins et al., 2022) and eight for every 10,000 births in outpatient services (or 0.8 full-time days per thousand births) (Royal College of Psychiatrists, 2021, p. 56).
In Spain, concern for perinatal mental health has been increasing in recent years, at the professional, institutional, and political levels. Several regional mental health plans include among their objectives the improvement of perinatal mental health care, including the Community of Madrid, Catalonia, Cantabria, and Aragon (Servicio Cántabro de Salud [Cantabrian Health Service], 2022; Oficina Regional de Coordinación de Salud Mental y Adicciones -ORCSMyA [Regional Office for the Coordination of Mental Health and Addictions -ORCSMyA], 2023; Unidad de Coordinación de Salud Mental [Mental Health Coordination Unit], 2022). In the Community of Madrid, the Strategic Plan currently in force and the previous one raised perinatal and 0-3 mental health care as a strategic objective (ORCSMyA, 2018; 2023). In addition, in recent years, papers have been published on the experience of specific programs in hospitals in the region (Cuéllar-Flores & Valle, 2017; Olza & Palanca, 2012), and the development of new programs has recently been announced (Tragacete, 30 March 2023; Community of Madrid, 12 September 2022; Mateos, 2 February 2023).
However, there are no censuses or lists of hospitals that carry out this type of program in the region, nor are their characteristics known. For this reason, the objective of this study was to identify the main programs of perinatal psychological care and care during the first thousand days of life in the hospitals of the Madrid Health Service, and to describe their organizational and care characteristics.
Method
The authors contacted at least one clinical psychology professional in 18 of the 24 hospitals of the Madrid Health Service with an obstetrics and gynecology (maternity) service and conducted a survey with open-ended questions via email on: 1) the existence of specific clinical psychology programs/consultations/care activities in perinatal mental health in the hospital where they work; 2) identification of the activities carried out, the context in which they are provided, and referral criteria; and 3) requesting to establish contact with at least one of the professionals involved in the program. This contact was made through an active search in our professional social networks (open instant messaging groups formed by more than 400 clinical psychology professionals in the Community of Madrid) and personal social networks.
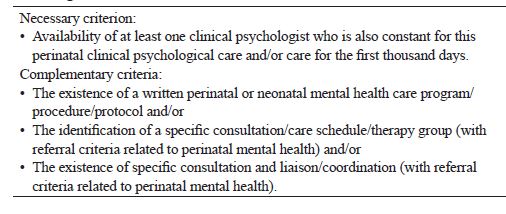
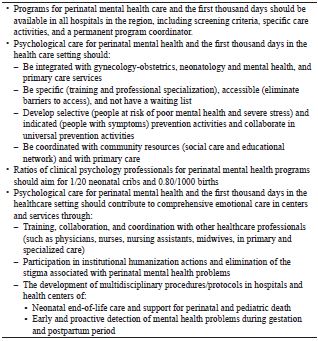
It is important to point out that in primary care in the Community of Madrid there is currently no specific clinical psychology care for the perinatal period. On the other hand, all the hospitals in the public network have interconsultation and liaison programs dependent on the mental health services, and they can receive interconsultations to attend patients during the perinatal period. The same can be said about the mental health centers, which are specialized level, and attend people with mental disorders, including people during the perinatal period. However, in this study we wanted to identify specific programs in perinatal mental health. The criteria we have used to define what we consider to be a perinatal clinical psychology and/or first thousand days care program are shown in Table 1. When only the necessary criterion is met, as well as just one of the complementary criteria, it has been considered a partial program.
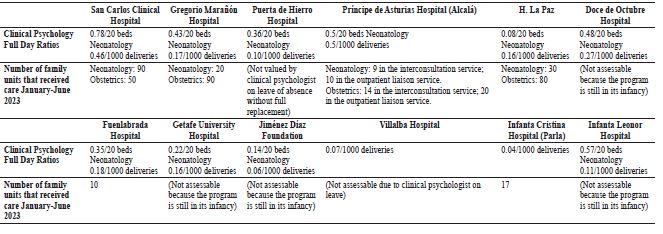
The organization, activities, and human resources of each program have been described. Ratios of clinical psychologists per delivery and neonatology cribs have also been calculated.
Results
Twelve hospitals of the Madrid Health Service were identified as having complete or partial programs (Table 1) of perinatal clinical psychology.
Tables 2 and 3 show a summary of the main characteristics of the perinatal clinical psychology and care programs for the first thousand days of life identified in this study.
Perinatal Clinical Psychology Programs and During the First Thousand Days of Life in High-Complexity Hospitals of the Madrid Health Service
The Hospital Clinic San Carlos has two programs in alliance and coordinated in perinatal and neonatal mental health care, the Neonatal Clinical Psychology Program of the Neonatology Service for more than 35 years (Cuellar-Flores & Valle, 2017) and the Perinatal Mental Health Interconsultation and Liaison Program of the Psychiatry and Mental Health Service in Gynecology-Obstetrics since 2021. The main activities are individual/couple/family psychological care for people undergoing assisted reproduction, pregnant women, mothers and babies in postpartum, and perinatal and neonatal bereavement, families of hospitalized neonates, and outpatient follow-up of these same families and their children up to two years of age.
The Perinatal Mental Health Interconsultation and Liaison Program of the Hospital General Universitario Gregorio Marañón offers psychological and/or psychiatric support and follow-up to families in Neonatology and Obstetrics during admission and on an outpatient basis. Psychological intervention includes individual, group, and/or family care. It is also provided to couples undergoing assisted reproduction, as well as couples facing prenatal diagnosis of malformation or syndromes, difficulties in postpartum or during early parenting with emotional and functional repercussions. There is a specific subprogram for dealing with perinatal bereavement, as well as for the health personnel involved, and group or individual intervention for families in the process of a new pregnancy, following a perinatal loss.
The initiation of the Perinatal Mental Health Interconsultation and Liaison Program at Hospital Puerta de Hierro (Majadahonda) has been previously described (Olza & Palanca, 2012; Olza et al., 2014). It was first developed in 2009 and since 2018 a new program was launched with psychological/psychiatric support during pregnancy and postpartum, in neonatology and in perinatal bereavement. Three psychotherapeutic groups have been developed: care for pregnant women (with a heterogeneous profile), care for postpartum mothers and babies (at risk of postpartum depression, posttraumatic symptomatology, and/or difficulties in bonding), and care for perinatal bereavement. It also responds to interconsultations that are requested individually.
The Perinatal Mental Health Interconsultation and Liaison Program of La Paz Hospital attends pregnant women, puerperal women, and families in Neonatology, after fetal death before birth or neonatal mortality, risk pregnancies due to fetal diagnosis or psychopathology in the mother, during hospitalization and in outpatient consultations. Also, neurodevelopmental monitoring and assessment is performed on neonates at biological risk up to two years of age.
The Child and Adolescent Mental Health Unit of the Hospital Universitario 12 de Octubre has a Perinatal Mental Health Program, called "1000 First Days Program" (for care from pregnancy to two years of age of the baby), which offers support and follow-up by a multidisciplinary team (clinical psychology, psychiatry, social work, and pediatric nursing) to women with perinatal losses, pregnant women, puerperal women, and families with newborns admitted to Neonatology. This program receives referrals from the Gynecology-Obstetrics and Neonatology Services. This intervention is part of an Interconsultation and Liaison Program, with post-home discharge outpatient consultations. Care is provided in the form of individual/family consultations, with plans to start psychotherapeutic groups in the coming months.
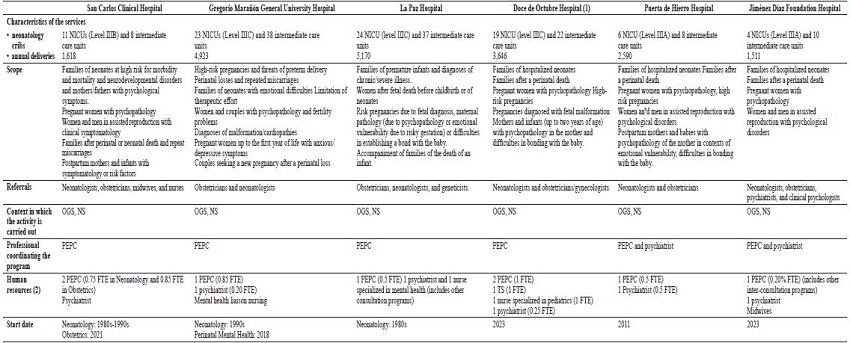
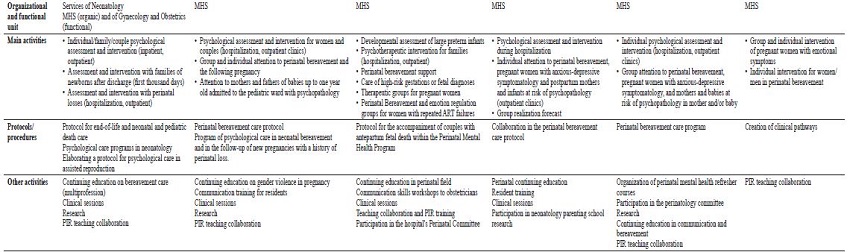
Note. High complexity hospitals.* 2020 data http://observatorioresultados.sanidadmadrid.org/HospitalesDatosGeneralesTabla.aspx?ID=86; (1) This program is currently being initiated, the information provided is part of the proposal to be developed; (2) Full-time equivalent days (FTE); NICU: Neonatal Intensive Care Unit, the levels correspond to the classification by complexity -Pérez-Muñuzuri et al., 2023; OGS: Obstetrics-Gynecology Service; NS: Neonatology Service; PEPC (in Spanish): Specialist Psychologist in Clinical Psychology; MHS: Mental Health Service; PIR (in Spanish): Psychologist Resident Intern
Clinical Psychology Programs for Perinatal and First Thousand Days of Life in Medium and low Complexity Hospitals of the Madrid Health Service
The Perinatal Mental Health Interconsultation and Liaison Program of the Hospital de Getafe has three programs of neonatal, perinatal, and postnatal clinical psychology. The first program was developed in 2008 (García-Villanova et al., 2013). Preterm infants born before 32 weeks of gestation and their families were included in the early care evaluation and follow-up program. In 2021, families in perinatal bereavement (from 22 weeks of gestation) or neonatal bereavement began to be attended in interconsultation. As of March 2023, the presence of clinical psychology in the hospital was expanded, and two programs for perinatal and postnatal care were launched. The first program treats pregnant women with affective and/or anxious symptoms who are being followed up in Obstetrics or admitted to the maternity ward. Finally, when the perinatal or neonatal psychology program detects a situation of parental emotional vulnerability that may affect parenting and parent-baby bonding, outpatient follow-up is offered until the baby is 2-3 years old.
The Perinatal Mental Health Interconsultation and Liaison Program of the Príncipe de Asturias Hospital (Alcalá de Henares) is integrated as one of the liaison programs of the Interconsultation Service. The team is multidisciplinary and is staffed by a psychiatrist, two adult clinical psychologists, and a child and adolescent clinical psychologist. There is no professional dedicated exclusively to the program, as all of them share the activity with the rest of the liaison processes. The process has been in the implementation period since 2013 (with the start of systematic care in Neonatology by the child and adolescent clinical psychologist), with the incipient development of the program beginning in 2022. None of the activities planned for the future have yet been implemented, including a psychotherapeutic group for families with psychological difficulties in early parenting. At present, individual and family care is aimed at patients with psychological care needs in fertility treatments, pregnancy (situations of perinatal pathology and severe mental disorder), childbirth, and postpartum, as well as perinatal bereavement in individual, family, and group format until the patient is discharged or referred.
In addition, there are partial perinatal clinical psychology programs in other hospitals in the Community of Madrid. Examples include the Fuenlabrada Hospital (perinatal bereavement care and its planned extension to neonatology families in an interconsultation program), the Villalba Hospital (perinatal bereavement group and agenda in the Mental Health Center), and the Infanta Cristina Hospital in Parla (specific perinatal mental health consultation and perinatal bereavement group in the Mental Health Center). Other hospitals are planning to start specific activities or expand them, such as the Infanta Leonor (individual and family psychological care for high-risk pregnant women and puerperal women with perinatal psychopathology and families after perinatal bereavement in an interconsultation program, with plans to initiate a perinatal bereavement group) and the Fundación Jiménez Díaz (psychoemotional care group during pregnancy and clinical pathways in an interconsultation program).
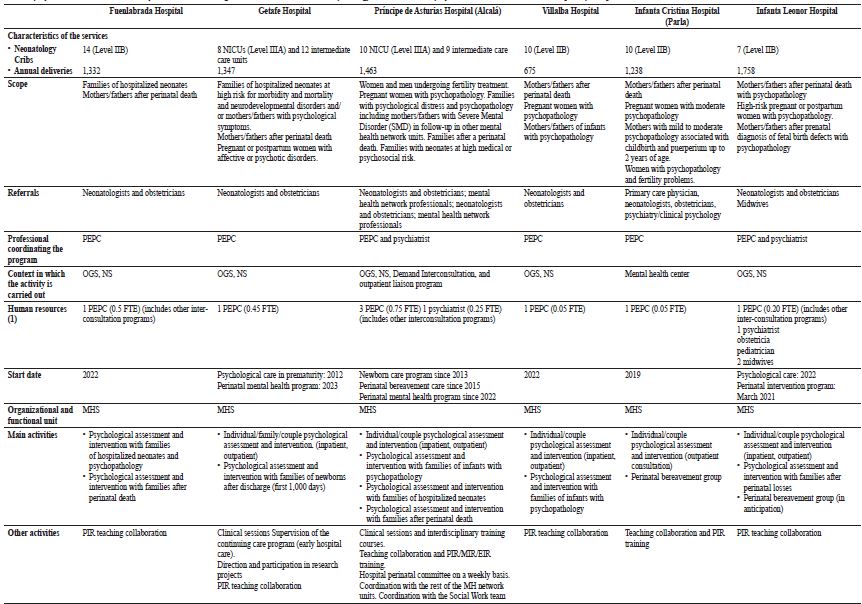
Note. * Data 2020 http://observatorioresultados.sanidadmadrid.org/HospitalesDatosGeneralesTabla.aspx?ID=86; (1) Full-time equivalent days (FTE); NICU: Neonatal Intensive Care Unit, the levels correspond to the classification by complexity -Pérez-Muñuzuri et al., 2023; OGS: Obstetrics-Gynecology Service; NS: Neonatology Service; PEPC (in Spanish): Clinical Psychology Psychologist; MHS: Mental Health Service; PIR (in Spanish): Resident Psychologist Intern; MIR (in Spanish): Resident Medical Intern; EIR (in Spanish): Resident Nurse Intern
Table 4 shows the ratios of clinical psychologists and the volumes of care for the programs described above.
Conclusions
In the Community of Madrid, most high complexity public hospitals (Observatorio de Resultados del Servicio Madrileño de Salud, revised 2023) have specific perinatal clinical psychology programs. Hospitals of medium and low complexity are also gradually incorporating this type of program, albeit through partial programs. In general, there is a consolidation of specialized psychological care in perinatal care (e.g., La Paz, Clínico San Carlos, Gregorio Marañon, and Puerta de Hierro Hospitals) and its expansion or extension (e.g. Doce de Octubre, Infanta Cristina, Fundación Jiménez Díaz, and Getafe Hospitals). On the other hand, all hospitals in the region with level IIIB and IIIC (or high complexity -Pérez-Muñuzuri et al., 2023) neonatology services have specific perinatal and neonatal mental health interconsultation and liaison programs.
Almost all of the programs described depend organizationally on the psychiatry and mental health service of the hospitals, although most of them are carried out through interconsultation programs and outpatient consultations within the obstetrics and neonatology services of the hospital. The recommendations of guidelines and expert groups (Austin et al., 2017; NICE, 2018; WHO, 2022), also in Spain (Conecta Perinatal, 2023; Rodríguez-Muñoz et al., 2023) are concerned with incorporating specific and integrated programs in maternal and child services, using clinical psychology professionals, with the objectives of improving the training of professionals, prevention, detection (and underdiagnosis), and in general, intervention in perinatal mental health problems. In Spain, and therefore in the Community of Madrid, mental health centers offer psychological assessments and interventions to people with mental disorders. However, the ordinary waiting lists of these centers (Cuéllar-Flores et al., 2022) are incompatible with adequate early care during this period, in addition to the fact that the preventive nature of the approach may be compromised as it is not integrated with maternal and child services and primary care. Moreover, if there are no programs with defined referral criteria, the risk of underdetection increases (Rodríguez-Muñoz et al., 2023; WHO, 2022). From the point of view of the authors, this integration must be carried out at both the primary and specialized care levels, with a phased model of intervention (Atkins et al., 2022). Not intervening has a high cost, both at an emotional level, due to the consequences it generates, as well as in economic terms for the healthcare system (Bauer et al., 2014).
The majority of referrals to the programs are made by physicians, with the possibility of referral from nursing being a minority. This responds to the traditional organization of requests for consultation in Spanish hospitals, and possibly also to the work overload of the professionals who develop these programs.
In this study we have been able to identify important differences in terms of the ratio of professionals, so that there are hospitals in which it is well below the recommended ratio (Atkins et al., 2022; Royal College of Psychiatrists, 2021), which translates into overloaded care and lower quality care in terms of frequency. Therefore, the data indicate that geographic barriers to access to specific perinatal mental health care exist in the region. Depending on where a person lives, specialized psychological care will be more or less accessible (taking into account the ratio of professionals) or more or less specialized (since there are hospitals that do not have specific programs).
Half of the hospitals have complete programs and the other half have only partial programs. The activities carried out cover direct patient care, all of them individually, but it is also offered in groups in four hospitals. Training and teaching activities and collaboration with the organization are also carried out. In six hospitals, written programs/procedures/protocols have been developed that can contribute to reducing unnecessary variability in clinical practice. On the other hand, most of the programs are developed and coordinated by a single clinical psychology professional (except for in three hospitals).
Based on the analysis of the characteristics of the programs, as well as the literature review and the experience of the authors, we have developed a set of recommendations for good practices in perinatal clinical psychology and care for the first thousand days (Table 5). Quality perinatal mental health care, in addition to being integrated and specific, should be coordinated with community resources, and have a phased prevention approach (Austin et al., 2017).
Among the limitations of this work is that it is a descriptive and incidental study, dependent on the information provided by the people contacted; it does not use a systematic procedure. In addition, it was not possible to contact mental health professionals from four of the 20 hospitals in the region. Future perspectives include extending this descriptive study to the rest of the Autonomous Communities. Also to examine the programs in terms of health outcomes and patient experience. In addition to studies on the efficacy of perinatal mental health interventions, studies of effectiveness, quality indicators (e.g. accessibility, appropriateness), and health outcomes of the interventions are needed.
In short, although the field of perinatal mental health care is currently being strengthened (several hospitals are opening partial or complete mental health programs), there is still much room for improvement. In the SERMAS public network, necessary and relevant work is being carried out for psychological care during the perinatal period, which has experienced an important boost in recent years and which must have a focus on consolidation and, above all, growth.
References
Atkins, A., Barr, K., Butterworth, R., Chilvers, R., Cole, S., Cordwell, J., D’Urso, A., Evans, D.,Higgins, S., & Marsh, A. (2022). Psychology Staffing on the Neonatal Unit-Recommendations for Psychological Provision’ ODN Psychology Leads July 2022. https://acpuk.org.uk/member-networks/psychology-staffing-on-the-neonatal-unit/
Austin, M., Highet, N., & The Expert Working Group. (2017). Mental health care in the perinatal period: Australian clinical practice guideline. http://cope.org.au/about/review-of-new-perinatal-mental-health-guidelines/
Bauer, A., Parsonage, M., Knapp, M., Iemmi, V., & Adelaja, B. (2014). The costs of perinatal mental health problems. Centre for Mental Health and London School of Economics. https://eprints.lse.ac.uk/59885/1/__lse.ac.uk_storage_LIBRARY_Secondary_libfile_shared_repository_Content_Bauer%2C%20M_Bauer_Costs_perinatal_%20mental_2014_Bauer_Costs_perinatal_mental_2014_author.pdf
Bauer, A., Pawlby, S., Plant, D. T., King, D., Pariante, C. M., & Knapp, M. (2015). Perinatal depression and child development: exploring the economic consequences from a South London cohort. Psychological Medicine, 45(1), 51-61. https://doi.org/10.1017/s0033291714001044
Besteiro, E. M., Aliaga, M. T., Pineda, M., Alegre, J. M., Berlanga, J. F., & Martín, P. B. (2001). La depresión postparto: un estudio exploratorio con una muestra de mujeres valencianas [Postpartum depression: an exploratory study with a sample of Valencian women]. Revista de Psicopatología y Psicología Clínica, 6(1), 37-48.
Burden, C., Bradley, S., Storey, C., Ellis, A., Heazell, A. E., Downe, S., ... y Siassakos, D. (2016). From grief, guilt pain and stigma to hope and pride-a systematic review and meta-analysis of mixed-method research of the psychosocial impact of stillbirth. BMC pregnancy and childbirth, 16, 1-12.
Burgio, S., Polizzi, C., Buzzaccarini, G., Laganà, A. S., Gullo, G., Perricone, G., ... & Alesi, M. (2022). Psychological variables in medically assisted reproduction: a systematic review. Menopause Review/Przegląd Menopauzalny, 21(1), 47-63. https://doi.org/10.5114/pm.2022.114404
Comunidad de Madrid [Community of Madrid] (12 September 2022). La Comunidad de Madrid lanza una iniciativa pionera para garantizar la salud física y mental de madres e hijos durante sus tres primeros años de vida [The Community of Madrid launches a pioneering initiative to guarantee the physical and mental health of mothers and children during their first three years of life]. .https://www.comunidad.madrid/noticias/2022/09/12/comunidad-madrid-lanza-iniciativa-pionera-garantizar-salud-fisica-mental-madres-e-hijos-tres-primeros-anos-vida
Conecta Perinatal (2023). Mejorar el cuidado de la salud mental perinatal. Fundamentos, propuestas y peticiones. [Improving perinatal mental health care. Rationale, proposals, and requests] Conecta Perinatal. https://conectaperinatal.com/pdf/ASMI_Memoradum_13sep2022_.pdf
Cuéllar-Flores, I., & Valle Trapero, M. (2017). Programa de Atención Psicológica en Neonatología: Experiencia del Hospital Clínico San Carlos de Madrid [Psychological Care Program in Neonatology: Experience of the Hospital Clínico San Carlos de Madrid]. Revista Clínica Contemporánea, 8(3), e28. https://doi.org/10.5093/cc2017a18
Cuéllar-Flores, I., Garzón, L. F., Félix-Alcántara, M. P., Olivares, B. M., Vega Rodríguez, I. de la, González, M. F., ... & Belmonte, M. J. M. (2022). Indicadores asistenciales y estándares de calidad asistencial para la psicología clínica en los centros de salud mental del Sistema Madrileño de Salud evaluados por sus profesionales [Care indicators and care quality standards for clinical psychology in the mental health centers of the Madrid Health System evaluated by their practitioners]. Apuntes de Psicología, 40(2), 71-86. https://doi.org/10.55414/ap.v40i2.1414
García-Villanova, F., Cuéllar-Flores, I., Eimil, B., & Palacios, I. (2013). El estrés materno en la organización del vínculo madre-bebé prematuro de bajo peso [Maternal stress in the organization of the low birth weight preterm mother-baby bond]. Clínica Contemporánea, 4(2), 171-183. https://doi.org/10.5093/cc2013a14
Goodman, J. H., & Tyer-Viola, L. (2010). Detection, treatment, and referral of perinatal depression and anxiety by obstetrical providers. Journal of Women's Health, 19(3), 477-490. https://doi.org/10.1089/jwh.2008.1352
Hynan, M. T., Mounts, K. O., & Vanderbilt, D. L. (2013). Screening parents of high-risk infants for emotional distress: rationale and recommendations. Journal of Perinatology, 33(10), 748-753. https://doi.org/10.1038/jp.2013.72
Mateos, A. (2 February 2023). Madrid refuerza la asistencia en salud mental durante el embarazo. [Madrid strengthens mental health care during pregnancy] Redacción Médica. https://www.redaccionmedica.com/secciones/parlamentarios/madrid-refuerza-la-asistencia-en-salud-mental-durante-el-embarazo-4071
National Institute for Health and Care Excellence (NICE). (2018). Antenatal and postnatal mental health: Clinical management and service guidance (CG192). https://www.nice.org.uk/guidance/cg192/resources/antenatal-and-postnatal-mental-health-clinical-management-and-service-guidance-pdf-35109869806789
Oficina Regional de Coordinación de Salud Mental y Adicciones -ORCSMyA [Regional Office for the Coordination of Mental Health and Addictions -ORCSMyA in Spanish] (2018). Plan Estratégico de Salud Mental de la Comunidad de Madrid 2018-2020 [Strategic Mental Health Plan of the Community of Madrid 2018-2020]. Madrid: Dirección General del Proceso Integrado de Salud. Servicio Madrileño de Salud. https://www.madrid.org/bvirtual/BVCM020214.pdf
Oficina Regional de Coordinación de Salud Mental y Adicciones -ORCSMyA [Regional Office for the Coordination of Mental Health and Addictions -ORCSMyA in Spanish] (2023). Plan Estratégico de Salud Mental y Adicciones 2022-2024 (PSMyA2022-2024) [Strategic Plan on Mental Health and Addiction 2022-2024]. Madrid: Dirección General del Proceso Integrado de Salud. Servicio Madrileño de Salud [Madrid Health Service]. https://www.comunidad.madrid/transparencia/sites/default/files/plan/document/bvcm050836-1.pdf
Olza Fernández, I., & Palanca, I. P. (2012). La experiencia del programa del Hospital Universitario Puerta de Hierro Majadahonda [The experience of the Hospital Universitario Puerta de Hierro Majadahonda program]. Cuadernos de Medicina Psicosomática y Psiquiatría de Enlace [Liaison Notebooks of Psychosomatic Medicine and Psychiatry], 101, 55-64.
Olza Fernández, I., Palanca, I., Rincón, I. G. V., Martínez, A. M. M., & Sales, A. C. (2014). La salud mental del recién nacido hospitalizado: psiquiatría infantil en neonatología [Mental health of the hospitalized newborn: child psychiatry in neonatology]. Cuadernos de Medicina Psicosomática y Psiquiatría de Enlace [Liaison Notebooks of Psychosomatic Medicine and Psychiatry], 109, 45-52.
Pérez-Muñuzuri, A., Boix, H., Sánchez-Redondo, M. D., Cernada, M., Espinosa-Fernández, M. G., González-Pacheco, N., & Luna, M. S. (2023). Niveles asistenciales en las unidades neonatales en España: Una visión actualizada para una nueva realidad [Levels of care in neonatal units in Spain: An updated view for a new reality]. Anales de Pediatría, 98(4), 301-307. https://doi.org/10.1016/j.anpedi.2023.02.009
Rodríguez-Muñoz, M., Rodríguez-Muñoz, M. F., Motrico, E., Miguez, M. C., Chaves, C., Suso-Ribera, C., Duque, A., García Salinas, M., Caparrós-González, R. A., Martin-Agudiez, N., Kovacheva, K., García-López, H., Vazquez-Batán, P., Peñacoba, C., & Osma, J. (2023). Perinatal depression in the Spanish context: Consensus report from the general council of psychology of Spain. Clínica y Salud, 34(2), 51-63. https://doi.org/10.5093/clysa2023a15
Royal College of Psychiatrists (2021). College Report CR232: Perinatal mental health services: Recommendations for the provision of services for childbearing women. https://www.rcpsych.ac.uk/improving-care/campaigning-for-better-mental-health-policy/college-reports/2021-college-reports/perinatal-mental-health-services-CR232
Servicio Cántabro de Salud [Cantabria Health Service] (2022). Plan de Salud Mental de Cantabria 2022-26 [Mental Health Plan of Cantabria 2022-26]. Servicio Cántabro de Salud. https://saludcantabria.es/uploads/pdf/consejeria/10-1191%20PLAN%20SALUD%20MENTAL%202022_WEB.pdf
Staneva, A., Bogossian, F., Pritchard, M., & Wittkowski, A. (2015). The effects of maternal depression, anxiety, and perceived stress during pregnancy on preterm birth: A systematic review. Women and Birth, 28(3), 179-193. https://doi.org/10.1016/j.wombi.2015.02.003
Tragacete, M. (30 March 2023). Madrid despliega un plan para atender a los bebés de familias en riesgo en sus primeros 1.000 días de vida [Madrid deploys a plan to care for babies from at-risk families in their first 1,000 days of life]. 20 Minutos. https://www.20minutos.es/noticia/5114668/0/el-12-de-octubre-y-la-paz-lanzan-un-proyecto-de-atencion-integral-a-familias-en-los-primeros-1-000-dias-de-vida-de-sus-bebes/
Unidad de Coordinación de Salud Mental. Dirección General de Asistencia Sanitaria Departamento de Sanidad Gobierno de Aragón [Mental Health Coordination Unit. General Directorate of Healthcare, Government of Aragon Department of Health] (2022). Plan de Salud Mental 2022-25 [Mental Health Plan 2022-25]. https://www.aragon.es/documents/20127/47401601/PLAN+DE+SALUD+MENTAL+DE+ARAG%C3%93N+2022-2025+d.pdf/63643efb-23fe-cfee-2e67-83e48d45b602?t=1673869931809
World Health Organization -WHO (2022). Guide for integration of perinatal mental health in maternal and child health services. Geneva: WHO https://apps.who.int/iris/rest/bitstreams/1467257/retrieve
Author notes
Correspondence: icuellarflores@gmail.com
Conflict of interest declaration