Original article
Infectious etiology and indicators of malabsorption or intestinal injury in childhood diarrhea
Etiología infecciosa e indicadores de malabsorción o daño intestinal en diarrea infantil
Infectious etiology and indicators of malabsorption or intestinal injury in childhood diarrhea
Biomédica, vol. 44, no. 1, pp. 80-91, 2024
Instituto Nacional de Salud
Received: 07 March 2023
Accepted: 19 February 2024
Published: 20 February 2024
Abstract
Introduction. : The multifactorial etiology of gastroenteritis emphasizes the need for different laboratory methods to identify or exclude infectious agents and evaluate the severity of diarrheal disease.
Objective. : To diagnose the infectious etiology in diarrheic children and to evaluate some fecal markers associated with intestinal integrity.
Materials and methods. : The study group comprised 45 children with diarrheal disease, tested for enteropathogens and malabsorption markers, and 76 children whose feces were used for fat evaluation by the traditional and acid steatocrit tests.
Results. : We observed acute diarrhea in 80% of the children and persistent diarrhea in 20%. Of the diarrheic individuals analyzed, 40% were positive for enteropathogens, with rotavirus (13.3%) and Giardia duodenalis (11.1%) the most frequently diagnosed. Among the infected patients, occult blood was more evident in those carrying pathogenic bacteria (40%) and enteroviruses (40%), while steatorrhea was observed in infections by the protozoa G. duodenalis (35.7%). Children with diarrhea excreted significantly more lipids in feces than non-diarrheic children, as determined by the traditional (p<0.0003) and acid steatocrit (p<0.0001) methods. Moreover, the acid steatocrit method detected 16.7% more fecal fat than the traditional method.
Conclusions. : Childhood diarrhea can lead to increasingly severe nutrient deficiencies. Steatorrhea is the hallmark of malabsorption, and a stool test, such as the acid steatocrit, can be routinely used as a laboratory tool for the semi-quantitative evaluation of fat malabsorption in diarrheic children.
Keywords: Diarrheal disease infectious+ children+ enterobacteria+ enterovirus+ Entamoeba histolytica+ Giardia duodenalis+ Blastocystis+ steatocrit.
Resumen
Introducción. : La etiología multifactorial de la gastroenteritis enfatiza la necesidad de usar diferentes métodos de laboratorio para identificar o excluir agentes infecciosos y evaluar la gravedad de la enfermedad diarreica.
Objetivo. : Diagnosticar la etiología infecciosa de la diarrea en niños y evaluar algunos marcadores fecales asociados con la integridad intestinal.
Materiales y métodos. : Se estudiaron 45 niños con enfermedad diarreica, en los cuales se evaluaron la presencia de enteropatógenos y los marcadores de malabsorción. Se analizaron las muestras fecales de 76 niños, mediante las pruebas de esteatocrito tradicional y esteatocrito ácido, para la cuantificación de la grasa.
Resultados. : Se observó diarrea aguda en el 80 % de los niños y diarrea persistente en el 20 %. De los individuos con diarrea, el 40 % fue positivo para enteropatógenos; los más diagnosticados fueron rotavirus (13,3 %) y Giardia duodenalis (11,1 %). Entre los pacientes infectados, la sangre oculta fue más evidente en aquellos portadores de bacterias patógenas (40 %) o enterovirus (40%), mientras que la esteatorrea se observó en infecciones por el protozoo G. duodenalis (35,7 %). Los niños con diarrea excretaron significativamente más lípidos en las heces que aquellos sin diarrea, según lo determinado por los métodos de esteatocrito tradicional (p<0,0003) y esteatocrito ácido (p<0,0001).
Conclusiones. : La diarrea infantil puede provocar deficiencias graves de nutrientes. La esteatorrea es distintiva de la malabsorción intestinal y puede detectarse mediante la estimación del esteatocrito ácido. Esta prueba podría utilizarse de forma rutinaria como una herramienta de laboratorio para la evaluación semicuantitativa de la malabsorción de grasas en niños con diarrea.
Palabras clave: Diarrea infecciosa, niños, enterobacterias, enterovirus, Entamoeba histolytica, Giardia duodenalis, Blastocystis rotavirus, esteatocrito.
Diarrhea is the third most common cause of illness in children in developing countries and accounts for about one-third of all hospitalizations among children under five years of age 1,2. Diarrhea is characterized by an increase in the number of bowel movements with excretion of soft or liquid feces. According to the period of diarrhea resolution, it can be classified as acute (up to two weeks), persistent (from two to four weeks), and chronic (episodes lasting more than four weeks) 2,3. In poor countries, diarrhea mainly affects individuals with reduced sanitation and hygiene conditions. It is often caused by infectious agents such as viruses, bacteria, or parasites, primarily transmitted through the fecal-oral route, carried by water or contaminated food 4-6.
Recently, a global pediatric diarrhea surveillance network enrolled children under five years, hospitalized with diarrhea from 28 low-income and middle-income countries, testing stool specimens by quantitative PCR for 16 infectious agents. Of the 5,465 samples tested, rotavirus was the leading cause of diarrhea (33.3%), followed by Shigella spp. (9.7%), norovirus (6.5%) and adenovirus (5.5%) 7. When considering only Central and South America, the most frequent pathogens in diarrheal disease were Shigella spp. (19.2%) and norovirus (22.2%) 7. Conversely, a molecular study conducted in Brazil showed that Escherichia coli was the leading infectious agent, detected in 71/110 (65%) children with diarrhea 8.
Inflammation due to intestinal infections may alter the microvillous architecture and physiology, leading to nutrient malabsorption, including lipids. If untreated, fat malabsorption may result in malnutrition, growth failure, and deficiencies of fat-soluble vitamins A, E, D, and K 9. Fat loss in feces can be evaluated using qualitative methods, such as SUDAN III 10 (rendering low accuracy) and quantitative or semi-quantitative tests 11. The gold standard test for fecal fat determination is the van de Kamer method, which consists of collecting the feces over 72 hours and determining the fecal fat extracted with petroleum ether. Because of the need for a high amount of fecal material, specific laboratory infrastructure, and the time-consuming protocol, the van de Kamer method use is not feasible in routine laboratories. Another method to evaluate the fat content in feces is the traditional or acid steatocrit 12. Some studies have reported its clinical applicability in the semi-quantitative assessment of steatorrhea degree in preterm infants and in several pediatric conditions, like coeliac disease, cystic fibrosis, and acute and chronic diarrhea 11-13.
This study aimed to evaluate the infectious etiology of diarrhea in hospitalized children to determine some indicators of intestinal malabsorption, and to analyze the performance of steatocrit tests (traditional and acid) in the fecal fat estimation of children with diarrhea.
Materials and methods
Study design and population
We conducted this cross-sectional study at the pediatric center of Professor Edgard Santos University Hospital and the Laboratório de Análises Clínicas of the Faculdade de Farmácia, Universidade Federal da Bahia, Brazil.
Children aged 0-5 years were selected by convenience sampling between 2016 and 2017 and grouped as follows: 45 inpatients with diarrheal illness (for pathogens and functional coprology evaluation) and 76 children, matched by age, exclusively for the latter comparison between traditional and acid steatocrit. The latter study sample consisted of 48 children (outpatients) with diarrhea and 28 apparently healthy children as a control group for fecal fat loss assessment. Children's families completed a questionnaire about socioeconomic and sanitation conditions, diarrhea duration, and other gastrointestinal symptoms.
Evaluation of fat, reducing substances and blood in fecal samples
The intestinal function of children with diarrhea included the steatocrit estimation for lipids detection, Benedict's reaction for reducing substances 14, and an immunochromatographic test for occult blood (Dialab® Gmbh, Wiener Neudorf, Austria). Traditional steatocrit was carried out through microcentrifugation of aqueous fecal homogenate, according to a previous report 15. The acid steatocrit method was similarly performed, except for perchloric acid addition (1/5 v/v) to the fecal homogenate 16. In this study, the steatocrit reference value was 3%, according to Cueto Rua, et al.13.
A control group for fat loss evaluation included 28 non-diarrheic children (described above in the Study design and population section), routinely seen at the Laboratório de Análises Clínicas. This group matched diarrheic patients' age and family income but lacked previous gastrointestinal diseases.
Identification of intestinal pathogens
Stool samples were analyzed using the following laboratory methods, depending to the infectious agent to be detected: a) direct examination, zinc sulfate (solution density of 1.18 g/ml), centrifugal flotation 17, sedimentation by centrifugation in water 18, and modified Ziehl-Neelsen staining 19 for helminths and protozoa diagnosis; b) ELISA for coproantigen detection of G, duodenalis, Cryptosporidium sp., and Entamoeba histolytica (Wampole II Cryptosporidium, Giardia II, and E. histolytica II, TECHLAB, Blacksburg, VA, USA); c) routine stool culture for pathogenic enterobacteria isolation, and d) rapid immunochromatographic test for rotavirus and adenovirus detection (RIDA® Quick Rotavirus / Adenovirus Combi, Germany), according to manufacturer's instructions.
Statistical analysis
We performed the statistical analysis with the GraphPad InStat program (GraphPad Software, Inc., San Diego, California, USA). We used the chi square test to analyze frequencies of infections by enteric pathogens, intestinal malabsorption markers or injury, and steatorrhea in children discriminated by the method. For steatocrit performance, we compared the values of eliminated fat by children from diarrhea and asymptomatic groups using the Student t test. A probability value under 0.05 was considered statistically significant.
Ethical considerations
The Research Ethics Committee of the Universidade Federal da Bahia, Escola de Enfermagem, approved this study, protocol # 907.867. We sent all laboratory results to the children's parents. Participants who tested positive for pathogenic intestinal microorganisms were treated appropriately by their respective pediatricians.
Results
Evaluation of intestinal infections, other gastrointestinal symptoms, and malabsorption markers or damage in children with diarrhea
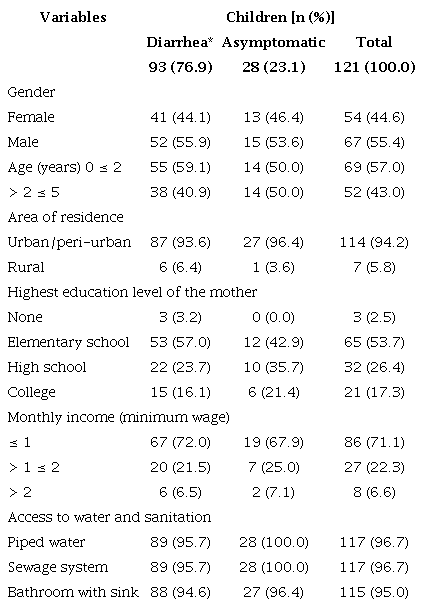
All examined children used public health services and came from low-income families, with 71.1% receiving up to one minimum Brazilian wage (around USD$ 260,00 per month), and only 26.4% of their parents had completed or were attending high school (table 1). Despite the low family income, most children (>95.0%) had basic sanitation conditions and access to piped water in their residences, which is compatible with inhabitants of urban and peri-urban areas (94.2% of residential areas).
Among the 45 children hospitalized with diarrheal disease, 36 (80%) presented acute. and 9 (20%) persistent diarrhea at the time of the fecal sample collection (table 2). Of the 45 children, 18 (40.0%) were infected by enteric pathogens. Intestinal viruses predominated (15.6%), followed by protozoa (13.3%) and enterobacteria (11.1%) (table 2). Single infections by rotavirus were more frequently detected (5/7; 71.4%; p<0.05) than adenovirus (1/7; 14.3%), with one child co-infected with the two enteroviruses. The stool culture revealed five children (11.1%) positive for pathogenic enterobacteria (table 2). Most children with diarrhea diagnosed with parasitic infections had G. duodenalis (5/6; 83%; (p<0.05). Four children had single infections, and one was coinfected with E. histolytica. One child presented Blastocystis spp. in feces (table 2). We observed other symptoms besides diarrhea in infected and noninfected individuals. Among the 18 children positive for infectious agents, the cases with fever were more related to the presence of enterovirus, vomiting events to bacteria, and coughing episodes to parasitic infections (table 2).
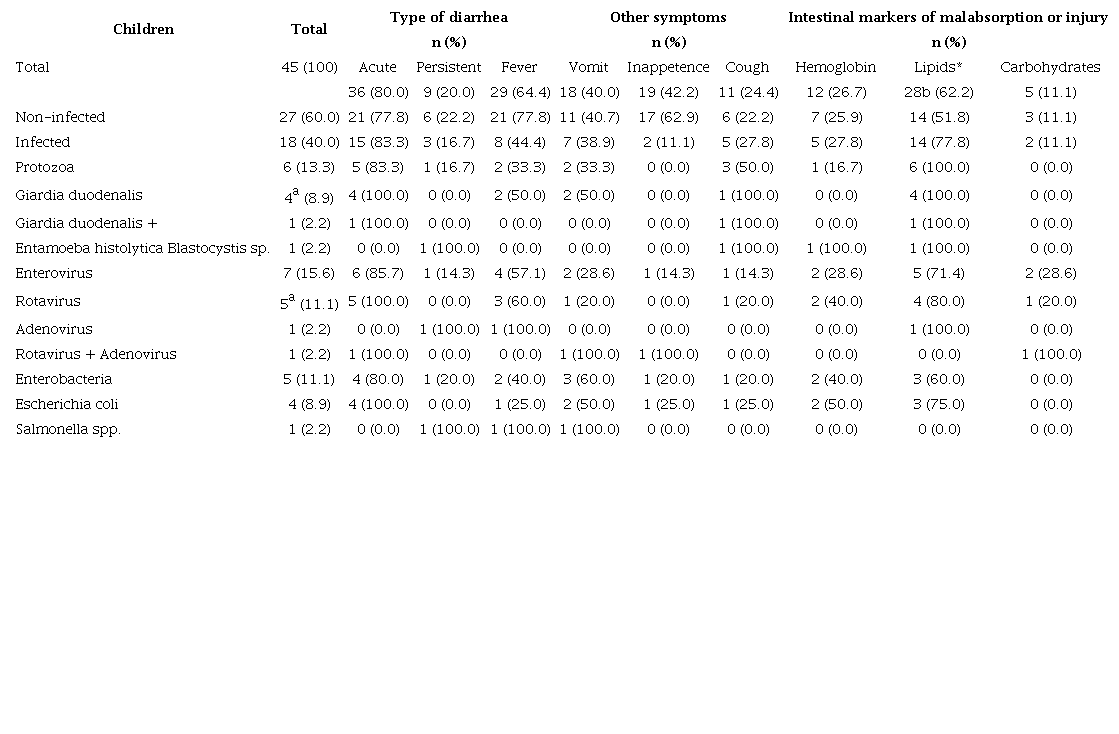
* Determined by steatocrit; cut-off limit = 3.0% of fecal fat (Cueto Rua, et al., 2006). Statistically significant differences between groups: ap<0.05 and bp<0.001, x2 test
Among the markers of intestinal injury, lipids loss in feces occurred more frequently in children with diarrhea (28/45; 62.2%) compared to hemoglobin loss (12/45; 26.7%) or carbohydrates (5/45; 11.1%; p<0.001) (table 2). Steatorrhea was proportionally more frequent in infected individuals (14/18; 77.8%) than in non-infected individuals (14/27; 51.8%), although without statistical significance (p>0.05). There were no differences in the frequency of fecal occult blood of children infected or not by intestinal pathogens. Five children tested positive for carbohydrates in feces. Of these, two were infected by enterovirus (table 2).
Comparison between ratios of fecal fat loss measured by traditional and acid steatocrit in children with diarrhea
Some authors have reported greater efficacy of fecal fat extraction in acidic media 16 for the semi-quantitative determination of fat loss in feces (acid steatocrit). Thus, we compared the traditional steatocrit with the acid steatocrit in 48 samples from children with diarrhea using other samples than those used to assess infectious etiology since previous material was insufficient to perform various tests or, in some cases, inadequately preserved for routine stool culture.
As controls, we used 28 fecal samples from healthy children to evaluate the fecal fat rate. The children with diarrhea had a mean of 5.59% for traditional steatocrit and 6.02% for acid steatocrit (median of 3.76% and 4.94%, respectively). Fecal samples from the asymptomatic children, used as controls, presented a mean of 2.15% for traditional steatocrit and 2.52% for the acid one (figure 1).
The observed steatocrit rates were statistically different between the diarrheic and asymptomatic groups, both by traditional (p<0.0003) and acidic method (p<0.0001) (figure 1). Percentages of fecal fat detected by the acid steatocrit method were 16.7% higher than those obtained by the traditional. Nonetheless, within the same group of children (diarrheic or asymptomatic), we did not observe statistical significance between the fat values obtained by traditional or acid steatocrit.
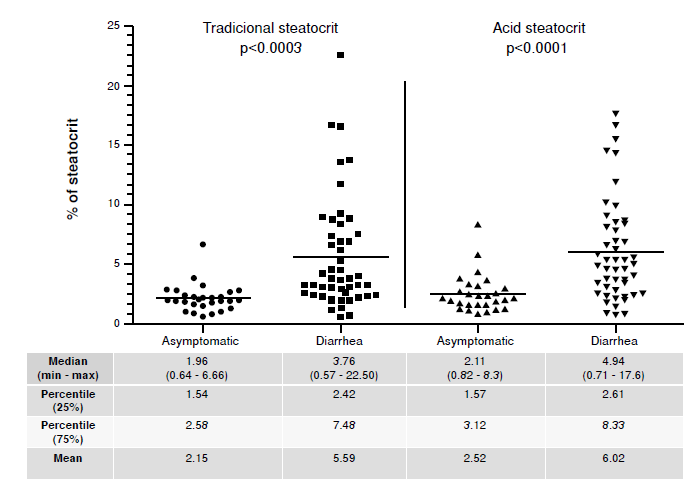
Figure 1
Comparison between traditional and acid steatocrit rates of fecal samples from children with diarrhea (n=48) and asymptomatic (n=28)
Similar to steatocrit rates, the frequency of children with steatorrhea in the diarrheal disease group compared to asymptomatic children was also significant, regardless of the steatocrit method used, if traditional (p<0.00001) or acid (p<0.0001) (table 3). Considering a normal reference value up to 3%, 32/48 (66.7%) diarrheic children were positive by the traditional and 35/48 (72.9%) by the acid steatocrit method, while 3/28 (10.7%) and 7/28 (25%) asymptomatic children were positive by the traditional and acid methods, respectively (table 3). Although we noticed a slight increase in the frequency of children with steatorrhea using the acid method, this was neither statistically significant for the diarrhea (p=0.656) nor the asymptomatic group (p=0.295) (table 3).
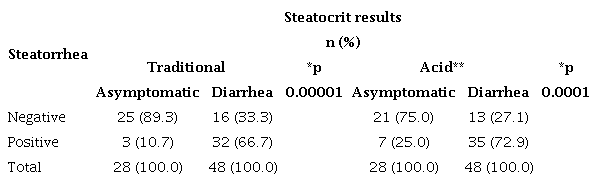
Positivity for fecal fat loss by steatocrit (reference value ≥ 3%) * p-value comparing steatorrhea positivity between children with and without diarrhea ** No significant statistical difference was observed in the frequency of steatorrhea in children when detected by the acid steatocrit compared to the traditional method (p=0.295 for the asymptomatic group and p=0.656 for the diarrhea group).
Discussion
In the management of children with diarrhea, it is essential to establish the enteric segment affected, the mechanisms involved (physiopathology), the chronology of the diarrheal process (acute, persistent, or chronic diarrhea), and the potential enteritis infectious etiology 20. According to Andrade and Fagundes-Neto 21, the rates of progression from an acute episode to persistent diarrhea range from 3% to 28% in children under five years of age. This rate depends on numerous reasons, such as enteropathogenic agents isolated in feces, seasonality, geographic aspects, socioeconomic and educational conditions, and levels of environmental sanitation 21. In this study, we found nine cases of persistent diarrhea. Persistent or chronic diarrheal disease has a high impact on morbidity and mortality rates in pediatric populations in developing countries. More than 50% of diarrheal deaths in these places are associated with persistent diarrheal syndrome 2,5.
In developing countries, low socioeconomic conditions are usually linked to gastrointestinal infections caused by parasites, viruses, and bacteria, especially during childhood 22,23. In this study, the analysis of the socioeconomic aspects of the children with diarrhea showed that they were from families with low educational and income levels, both variables usually associated with intestinal pathogen infections in children 23-25.
Rotavirus is considered the most important etiological agent of severe diarrhea in childhood worldwide 26. In this work, 7/45 (15.6%) diarrheic children were diagnosed with enteroviruses, predominating rotavirus infections. Of the five children testing positive for fecal blood, two had rotavirus. Other studies conducted with pediatric patients with diarrhea in the northeastern region of Brazil showed high frequencies (up to 19%) of rotavirus, with the presence of fever, vomiting, and dehydration 27,28. This virus has a higher occurrence in children between four and nine months of age, making it one of the most frequent causes of acute abdominal pain in this age group. One study measuring the occurrence of adenovirus in fecal samples from children with acute gastroenteritis in Belém demonstrated 3.7% (13/380) positivity for adenoviruses 29, a similar frequency found in our study. It is important to note that we did not perform norovirus diagnosis nor use molecular biology tools to detect rotavirus, which could increase the positivity rate of enterovirus infections in the population studied. Norovirus is considered the second cause of gastroenteritis after rotavirus infection, and epidemiological studies show that norovirus infection is frequently associated with outpatient consultations due to gastrointestinal symptoms 30.
Infections by helminths and intestinal protozoa cause a wide range of symptoms associated with the gastrointestinal tract, depending on host demographic, socioeconomic, and immunological factors of the hosts 31,32. In this work, six children with diarrhea had infections by intestinal protozoa. Four of these children had single infections by G. duodenalis, two reported episodes of vomiting and fever (symptoms that can be associated with giardiasis), and one child had a concomitant infection by G. duodenalis and E. histolytica. Belloto et al.(33 found G. duodenalis in 47 (15.16%) and E. histolytica in two (0.64%) of the 310 schoolchildren studied in São Paulo. Some reports have associated G. duodenalis infections with childhood diarrhea 21,34,35. However, studies developed by our group found G. duodenalis mostly in asymptomatic children, which seems more common in endemic countries such as Brazil 36,37, and only one child with persistent diarrhea had a single infection by Blastocysts sp. Most Blastocysts sp. infected patients around the world are asymptomatic, but when symptoms persist without other causes, anti-parasite treatment is recommended 38.
Epidemiological studies on species-specific Entamoeba infections are limited due to the morphological resemblance of Entamoeba histolytica with non-pathogenic E. dispar and E. moshkovskii. Specific methods based on molecular techniques like PCR and fecal detection of E. histolytica antigens are required to make a reliable diagnosis of E. histolytica intestinal infections. A study in Pernambuco analyzed 213 stool samples, with 10 (4.7%) positive for E. histolytica/E. dispar/E. moshkovskii complex, but when tested by ELISA for E. histolytica antigens, all samples were negative 39.
Previous studies by our group in Salvador found 788/52,704 (3.4%) and 273/55,218 (0.49%) positive fecal samples for E. histolytica/E. dispar/E. moshkovskii complex by microscopic examination. The group randomly analyzed some amoeba-positive stools by PCR and ELISA. All of them were negative for E. histolytica and positive for E. dispar40. Moreover, the evaluation of specific antibodies in sera by ELISA detected a seropositivity of 8.9% (8/90). These results point out the absence or very low prevalence of E, histolytica in asymptomatic carriers in the evaluated population of Salvador, and the antibody production induced by E. dispar infections 40,41. Nonetheless, our study finding of E. histolytica in one child with diarrhea demonstrates the need for specific laboratory diagnosis of this parasite, even in areas with low transmission.
A study in Brazil with children groups reported an approximate frequency of 10% of diarrheic bacterial infections 42. This result is similar to that found herein (11.1%). Moura et al.43 evaluated 140 stools of diarrheic children in Pernambuco with socioeconomic conditions comparable to those of the population in our study in Salvador. They found 9 (6.4%) samples positive for enteropathogenic and invasive Escherichia coli and 3 (2.1%) for Salmonella spp. In this study, two of the four patients who tested positive for E. coli had blood in their stools. Furthermore, the child with Salmonella spp. had persistent diarrhea, fever, and episodes of vomiting, common symptoms of salmonellosis. Anal fissures are often related to fecal blood, followed by infectious diseases 44. However, none of the participating children presented anal fissures, as observed in medical records.
Among the 45 children with diarrheal disease, five excreted reducing substances in their feces: one had rotavirus infection, one adenovirus infection, and the remaining three were negative for enteric pathogens. Viral replication in the intestinal villi epithelium of the jejunum can induce a process of malabsorption, mainly due to a transient decrease of disaccharidases 14,45. Reducing substances present in stool indicates carbohydrate intolerance, usually secondary to a viral illness. On the other hand, the sugar loss in the feces of non-infected patients may be related to the timedecrease of the fecal bolus in the intestine due to the diarrheal process, generating a reduced absorption of several nutrients, including carbohydrates.
Fecal fat examination generally aims to establish a more objective diagnostic pattern of malabsorption origin (infectious, celiac, or other autoimmune diseases or cystic fibrosis) and in the therapeutic approach. Fecal fat loss estimation usually requires quantitative or semi-quantitative tests. The gold standard test for fecal fat quantitative determination is the van de Kamer test. However, despite its low cost, collecting all stools over 72 hours is inconvenient and difficult to perform with constipated patients, neonates, and infants. In addition, this method requires the infrastructure and reagents for fat extraction and quantification by chemical processes that are not always available in routine laboratories 15,46,47.
Despite the use of the traditional steatocrit method in the evaluation of fecal fat, this test also presents some limitations, such as: the reading of the fat layer when the patient is eliminating insignificant or even undetectable fat amounts, or the observer's inexperience in delimiting the layers for a proper reading of the fat rates. However, performing the technique in triplicate, correctly homogenizing the sample, centrifuging the material in a defined time 15, and even using an acidic media for a more effective fecal fat extraction, as reported 16, can reduce execution error.
In this study, we observed a significant difference in the rates of fat loss in children with diarrhea compared to the asymptomatic children. This effect was evident when using acid steatocrit (p<0.0001). Other authors reported fat malabsorption occurrence in children with diarrhea, as observed in this study 20,21,45. Due to the higher sensitivity of the acid steatocrit in contrast to the classic steatocrit, this method can be useful to rule out steatorrhea as a screening laboratory tool, avoiding subjecting patients to more laborious and timeconsuming techniques such as the van de Kamer test 16,47. It is worth mentioning the increased number of steatorrhea positive cases in asymptomatic children found in our study when using the acid method. A follow-up with consecutive determinations or a quantitative evaluation of fecal fat would be advisable to discard false positive cases of steatorrhea.
Infectious agents and dietary errors are the principal causes of diarrhea in children, and infections by enteropathogens are the most relevant etiology in developing countries 27,48. In this context, methods used to identify infectious agents and to study intestinal malabsorption markers in health services can help to diagnose intestinal diseases, to promote prompt treatment, and to improve prognosis in childhood. The multifactorial etiology of gastroenteritis emphasizes the need for different laboratory methods to identify or exclude infectious agents, to determine markers of intestinal malabsorption, and to evaluate the severity of diarrheal disease.
A determinant limitation of this study was the sample size to evaluate the different pathogens and intestinal integrity markers in children with diarrhea. Among the difficulties encountered, the most important was the reduced amount of feces collected from hospitalized children and their inadequate preservation until laboratory analysis, hampering the use of many samples during the study. Despite the small sample size, the obtained results were similar to those of other studies conducted in Brazil 27-29,34,35,40-42. Moreover, in another study carried out by our group, from January 2011 to June 2012, we analyzed parasitic infections in 151 children with diarrhea from Salvador and we found a relatively low frequency of Cryptosporidium (4.6%) and E. histolytica (3.3%), and the absence of Cyclospora cayetanensis and Cystoisospora belli18. Therefore, a larger sample size would be necessary to find any of these latter parasites in such a specific population.
In conclusion, this study highlights the importance of monitoring childhood diarrhea by different laboratory methods, including acid steatocrit measurement as an alternative tool for the semiquantitative evaluation of fecal fat.
References
Brandt KG, Antunes MMC, Silva GAP. Acute diarrhea: Evidence-based management. J Pediatr (Rio J). 2015;91(Supp.1):S36-43. https://doi.org/10.1016/j.jped.2015.06.002
Global Burden of Diseases, Injuries, and Risk Factors Study. Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the global burden of disease study 2016. Lancet Infect Dis. 2018;18:1211-28. https://doi.org/10.1016/S14733099(18)30362-1
Flórez ID, Niño-Serna LF, Beltrán-Arroyave CP. Acute infectious diarrhea and gastroenteritis in children. Curr Infect Dis Rep. 2020;22:4. https://doi.org/10.1007/s11908-020-0713-6
Pereira IV, Cabral IE. Diarréia aguda em crianças menores de um ano: subsídios para o delineamento do cuidar. Esc Anna Nery Rev Enferm. 2008;12:224-9. https://doi.org/10.1590/S1414-81452008000200004
Behera DK, Mishra S. The burden of diarrhea, etiologies, and risk factors in India from 1990 to 2019: Evidence from the global burden of disease study. BMC Public Health. 2022;22:92. https://doi.org/10.1186/s12889-022-12515-3
World Health Organization. Diarrhoeal disease. Accessed: 18 January 2023. Available at: Available at: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease
Cohen AL, Platts-Mills JA, Nakamura T, Operario DJ, Antoni S, Mwenda JM, et al. Aetiology and incidence of diarrhoea requiring hospitalisation in children under 5 years of age in 28 low-income and middle-income countries: Findings from the Global Pediatric Diarrhea Surveillance network. BMJ Glob Health. 2022;7:e009548. https://doi.org/10.1136/bmjgh-2022-009548
Merino VR, Nakano V, Delannoy S, Fach P, Alberca GGF, Farfan MJ, et al. Prevalence of enteropathogens and virulence traits in Brazilian children with and without diarrhea. Front Cell Infect Microbiol. 2020;10:549919. https://doi.org/10.3389/fcimb.2020.549919
Keller J, Layer P. The pathophysiology of malabsorption. Viszeralmedizin. 2014;30:150-4. https://doi.org/10.1159/000364794
_Khouri MR, Huang G, Shia YF. Sudan stain of fecal fat: New insight into an old test. Gastroenterol. 1989;96:421-7. https://doi.org/10.1016/0016-5085(89)91566-7
Maranhão HS, Wehba J. Steatocrit and Sudan III in the study of steatorrhea in children: Comparison with the van de Kamer method. Arq Gastroenterol. 1995;32:140-5.
Sugai E, Srur G, Vázquez H, Benito F, Mauriño E, Boerr LA, et al. Steatocrit: A reliable semiquantitative method for detection of steatorrhea. J Clin Gastroenterol. 1994;19:206-9. https://doi.org/10.1097/00004836-199410000-00007
Cueto Rua EA, Nanfito G, Guzmán L. La enfermedad celíaca. Ludovica Pediátr. 2006;8:85-99.
Castro-Rodriguez JA, Salazar-Lindo E, León-Barúa R. Differentiation of osmotic and secretory diarrhoea by stool carbohydrate and osmolar gap measurements. Arch Dis Child. 1997;77:201-5. https://doi.org/10.1136/adc.77.3.201
Phuapradit P, Narang A, Mendonça P, Harris DA, Baum JD. The steatocrit: A simple method for estimating stool fat content in newborn infants. Arch Dis Child. 1981;56:725-7. https://doi.org/10.1136/adc.56.9.725
Tran M, Forget P, van Den Neucker A, Strik J, van Kreel B, Kuijten R. The acid steatocrit: A much improved method. J Pediatr Gastroenterol Nutr. 1994;19:299-303. https://doi.org/10.1097/00005176-199410000-00007
Faust EC, D'antoni JS, Odom V, Miller MJ, Peres C, Sawitz W, et al. A critical study of clinical laboratory technics for the diagnosis of protozoan cysts and helminth eggs in feces I. Preliminary communication. Am J Trop Med. 1938;18:169-83.
Pacheco FT, Silva RK, Martins AS, Oliveira RR, AlcântaraNeves NM, Silva MP, et al. Differences in the detection of Cryptosporidium and Isospora (Cystoisospora) oocysts according to the fecal concentration or staining method used in a clinical laboratory. J Parasitol. 2013;99:1002-8. https://doi.org/10.1645/12-33.1
Henriksen SA, Pohlenz JF. Staining of cryptosporidia by a modified Ziehl-Neelsen technique. Acta Vet Scand. 1981;22:594-6. https://doi.org/10.1186/BF03548684
Semrad CE. Approach to the patient with diarrhea and malabsorption. Goldman's Cecil Medicine. 2012;1:895-913. https://doi.org/10.1016/B978-1-4377-1604-7.00142-1
Andrade JAB, Fagundes-Neto U. Diarréia persistente: ainda um importante desafio para o pediatra. J Pediatr (Rio J), 2011;87:199-205. https://doi.org/10.2223/JPED.2087
Motta MEFA, Silva GAP. Diarréia por parasitas. Rev Bras Saúde Mater Infant. 2002;2:117-27. https://doi.org/10.1590/S1519-38292002000200004
Pedraza DF, Queiroz D, Sales MC. Doenças infecciosas em crianças pré-escolares brasileiras assistidas em creches. Ciên Saúde Colet. 2014;19:511-28. https://doi.org/10.1590/1413-81232014192.09592012
Reis LB, Santos RS, Mota LH, Jesus JS, Oliveira JM, Andrade RS, et al. Enteroparasites, demographic profile, socioeconomic status and education level in the rural population of the Recôncavo of Bahia, Brazil. J Trop Pathol. 2019;48:197-210.
Ferreira ALC, Carvalho FF, Nihei OK, Nascimento IA, Shimabuku Junior RS, Fernandes RD, et al. Prevalence of intestinal parasites in children from public preschool in the Triple Border Brazil, Argentina, and Paraguay. ABCS Health Sci. 2021;46:e021205.
Burnett E, Parashar UD, Tate JE. Global impact of rotavirus vaccination on diarrhea hospitalizations and deaths among children <5 years old: 2006-2019. J Infect Dis. 2020;222:1731-9. https://doi.org/10.1093/infdis/jiaa081
Cauás RC, Falbo AR, Correia JB, Oliveira KMM, Montenegro FMU. Diarréia por rotavírus em crianças desnutridas hospitalizadas no Instituto Materno Infantil Prof. Fernando Figueira, IMIP. Rev Bras Saúde Mater Infant. 2006;6:77-83. https://doi.org/10.1590/S1519-38292006000500011
Silva ML, Souza JR, Melo MMM. Prevalência de rotavírus em crianças atendidas na rede pública de saúde do estado de Pernambuco. Rev Soc Bras Med Trop. 2010;43:548-51. https://doi.org/10.1590/S0037-86822010000500015
Muller ECA, Morais MAA, Gabbay Y, Linhares AC. Ocorrência de adenovírus em crianças com gastrenterite aguda grave na Cidade de Belém, Pará, Brasil. Rev Pan-Amaz Saúde. 2010;1:49-55. https://doi.org/10.5123/S2176-62232010000300007
Morillo SG, Timenetsky MCST. Norovírus: uma visão geral. Rev Assoc Med Bras. 2011;57:453-8. https://doi.org/10.1590/S0104-42302011000400023
Wale M, Gedefaw S. Prevalence of intestinal protozoa and soil transmitted helminths infections among schoolchildren in Jaragedo Town, South Gondar Zone of Ethiopia. J Trop Med. 2022;2022:ID 5747978. https://doi.org/10.1155/2022/5747978
Sebaa S, Behnke JM, Baroudi D, Hakem A, Abu-Madi MA. Prevalence and risk factors of intestinal protozoan infection among symptomatic and asymptomatic populations in rural and urban areas of southern Algeria. BMC Infect Dis. 2021;21:888. https://doi.org/10.1186/s12879-021-06615-5
Belloto MVT, Santos Junior JE, Macedo EA, Ponce A, Galisteu KJ, Castro E, et al. Enteroparasitoses numa população de escolares da rede pública de ensino do Município de Mirassol, São Paulo, Brasil. Rev Pan-Amaz Saúde. 2011;2:37-44. https://doi.org/10.5123/S2176-62232011000100004
Newman RD, Moore SR, Lima AAM, Nataro JP, Guerrant RL, Sears CL. A longitudinal study of Giardia lamblia infection in northeast Brazilian children. Trop Med Int Health. 2001;6:624-34. https://doi.org/10.1046/j.1365-3156.2001.00757.x
Wu Y, Yao L, Chen H, Zhang W, Jiang Y, Yang F, et al. Giardia duodenalis in patients with diarrhea and various animals in northeastern China: Prevalence and multilocus genetic characterization. Parasit Vectors. 2022;15:165. https://doi.org/10.1186/s13071-022-05269-9
Silva RKNR, Pacheco FTF, Martins AS, Menezes JF, Costa-Junior HR, Ribeiro TCR, et al. Performance of microscopy and ELISA for diagnosing Giardia duodenalis infection in different pediatric groups. Parasitol Int. 2016;65:635-40. https://doi.org/10.1016/j.parint.2016.08.012
Pacheco FTF, Silva RKNR, Carvalho SS, Rocha FC, Chagas GMT, Gomes DC, et al. Predominance of Giardia duodenalis. AII sub-assemblage in young children from Salvador, Bahia, Brazil. Biomédica. 2020;40:557-68. https://doi.org/10.7705/biomedica.5161
Ocaña-Losada C, Cuenca-Gómez JA, Cabezas-Fernández MT, Vázquez-Villegas J, Soriano-Pérez MJ, Cabeza-Barrera I, et al. Clinical and epidemiological characteristics of intestinal parasite infection by Blastocystis hominis, Rev Clin Española. 2018;218:115-20. https://doi.org/10.1016/j.rceng.2018.01.008
Dourado A, Maciel A, Aca IS. Ocorrência de Entamoeba histolytica/Entamoeba dispar em pacientes ambulatoriais de Recife, PE. Rev Soc Bras Med Trop. 2006;39:388-9. https://doi.org/10.1590/S0037-86822006000400015
Soares NM, Azevedo HC, Pacheco FTF, Souza JN, Del-Rey RP, Teixeira MCA, et al. A cross-sectional study of Entamoeba histolytica/dispar/moshkovskii complex in Salvador, Bahia, Brazil. Biomed Res Int. 2019;2019:7523670. https://doi.org/10.1155/2019/7523670
Santos FLN, Goncalves MS, Soares NM. Validation and utilization of PCR for differential diagnosis and prevalence determination of Entamoeba histolytica/ Entamoeba dispar in Salvador City, Brazil. Braz J Infect Dis. 2011;15:119-25. https://doi.org/10.1016/S1413-8670(11)70156-8
Franzolin MR, Alves RCB, Kellertânia R, Gomes TAT, Beutin L, Barreto ML, et al. Prevalência de Escherichia coli diarreica em crianças com diarréia em Salvador, Bahia, Brasil. Mem Inst Oswaldo Cruz. 2005;100:359-63. https://doi.org/10.1590/S0074-02762005000400004
Moura MR, Mello MJG, Calábria WB, Germano EM, Maggi RR, Correia JB. Frequência de Escherichia coli e sua sensibilidade aos antimicrobianos em menores de cinco anos hospitalizados por diarréia aguda. Rev Bras Saúde Mater Infant. 2012;12:173-82. https://doi.org/10.1590/S1519-38292012000200008
Lopes AIG, Trindade E, Pereira F, Antunes H, Dias JÁ, Ferreira R, et al. Gastrenterologia Pediátrica: aspectos práticos. Editor: Pereira F, SPED. Serviço de Gastrenterologia Pediátrica. Hospital Maria Pia. Centro Hospitalar do Porto, 2010. Accessed: 15 January 2023. Available: Available: https://www.sped.pt/images/Publicacoes SPED/LivroGastroPediatrica Jul10.pdf
Hendrawati LD, Firmansyah A, Darwis D. Macronutrient malabsorption in acute diarrhea: Prevalence and affecting factors. Paediatr Indones. 2005;45:207-10.
Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, Tilburg M. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterol. 2006;130:1527-37. https://doi.org/10.1053/j.gastro.2005.08.063
van der Neucker A, Kerkvliet EM, Theunissen PMVM, Forget PPH. Acid steatocrit: A reliable screening tool for steatorrhea. Acta Paediatr. 2007;90:873-5. https://doi.org/10.1111/j.1651-2227.2001.tb02448.x
Mendes PS, Ribeiro Junior HC, Mendes CM. Tendência temporal da mortalidade geral e morbidade hospitalar por doença diarreica em crianças brasileiras menores de cinco anos no período de 2000 a 2010. J Pediatr (Rio J). 2013; 89:315-25. https://doi.org/10.1016/j.jped.2012.10.002
Author's contributions:
Author notes
*Corresponding author: Márcia Cristina Aquino Teixeira, Av. Barão de Jeremoabo, N° 147, Campus Universitário de Ondina 40170-115, Salvador, Bahia, Brasil Telephone: +55 (71) 3 283 6950/6954 marciat@ufba.br
Conflict of interest declaration