Abstract:
Aim: To analyze acute glycemic, cardiovascular variables, and level of enjoyment (LE) in response to active video games (AVG) in adults.
Methods: Fourteen adults performed a 30-minute AVG session. Heart rate (HR), systolic (SBP) and diastolic (DBP) blood pressure, double product (DP) and blood glucose (BG) were recorded at rest, immediately after and at 30 minutes after AVG session. At the end of the session, participants reported the rating of perceived exertion (RPE, 6-20 scale) and LE (0-10 scale).
Results: Participants reached 55.5% HR reserve with high RPE (Mean=15). BG decreased (−10.3 mg·dL−1), and HR (+85 bpm), SBP (+23.8 mm Hg) and DP (+12852 mm Hg × bpm) increased immediately after the session and returned to resting levels after 30 minutes. DBP did not present statiscal changes over time. High LE levels were found (Mean=8.6).
Conclusion: A 30-minute AVG session at moderate-intensity was very enjoyable, effective in reducing blood glucose levels acutely and promote safe cardiovascular acute changes in adults.
Keywords:Physical ExertionPhysical Exertion,Diabetes MellitusDiabetes Mellitus,Blood pressureBlood pressure,Cardiovascular SystemCardiovascular System,MotivationMotivation.
Resumo:
Objetivo: Analisar glicemia aguda, variáveis cardiovasculares e nível de satisfação à prática (LE) de adultos saudáveis em resposta aos videogames ativos (AVG).
Métodos: Quatorze adultos realizaram uma sessão de AVG de 30 minutos. Frequência cardíaca (FC), pressão arterial sistólica (PAS) e diastólica (PAD), duplo produto (DP) e glicemia foram registrados em repouso, imediatamente após e 30 minutos após sessão de AVG. Ao final, os participantes relataram percepção subjetiva de esforço (PSE, escala 6-20) e LE (escala 0-10).
Resultados: Os participantes alcançaram 55,5% da reserva da FC e PSE elevada (Média=15). A glicemia reduziu (−10,3 mg·dL−1) e FC (+85 bpm), PAS (+23,8 mm Hg) e DP (+12852 mm Hg × bpm) aumentaram imediatamente após a sessão e retornaram aos valores de repouso após 30 minutos. A PAD não apresentou alterações significantes ao longo do tempo. Níveis elevados de LE foram encontrados (Média=8,6).
Conclusão: Uma sessão de 30 minutos de AVG em intensidade moderada reduziu a glicose sanguínea e promoveu alterações hemodinâmicas seguras e alto nível de satisfação em adultos.
Palavras-chave: Esforço Físico, Diabetes Mellitus, Pressão Arterial, Sistema Cardiovascular, Motivação.
Do 30 minutes of active video games at a moderate-intensity promote glycemic and cardiovascular changes?
30 minutos de vídeo game ativo a uma intensidade moderada promovem alterações glicêmicas e cardiovasculares?
Universidade Nove de Julho

This work is licensed under Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International.
Received: 22 May 2019
Accepted: 13 December 2019
Physical activity (PA) promotes cardiovascular (such as elevations on heart rate and blood pressure which stimulates post-exercise hypotension) and metabolic benefits (such as favorably change energy expenditure and oxygen uptake and improve energy intake of blood glucose)1. However, people in general not take part in considerable amounts of PA to attain positive psychophysical outcomes. PA is still a relatively underutilized strategy for the prevention, care, and management of numerous illnesses2,3. In general, an effective PA program must take into consideration a person’s interests, needs, environment, social contexts, and even the possibility of inclement weather.. Therefore, a successful intervention requires that the subject is motivated and quickly experiences a tangible effect on personal efforts4.
Although traditional aerobic and strength training has been recommended in exercise programs1, active video games (AVG) are becoming a popular form of PA, and they have been used to treat a wide range of chronic diseases and clinical disorders in different age groups and special population.. AVG are a genre of serious games and games for health with a high level of enjoyment (LE) to play it that requires body movement to move the game forward, assisting to improve fitness levels and develop motivation and self-efficacy for PA6,7,8. Despite AVG share common physiological responses with other forms of exercise6,9, little attention is given to blood glucose (BG) and other cardiovascular parameters in response to AVG, which could be an alternative to analyzing the physical effort at home.
Acute effects of AVG on glycemic control are not well studied, although some variables of exercise prescription, such as intensity and duration, could change it10, 11. A single bout of traditional aerobic exercise (30-60 min up to 60-70% of maximal oxygen consumption) increases glucose transporters (GLUT-4) translocation to the sarcolemmal membrane and can significantly lower plasma glucose levels12. However, a previous study with AVG did not show a significant acute reduction in BG levels, probably due to light intensity and short duration of the session (Wii Fit Running game), even when maximal oxygen uptake of healthy adults was controlled11. Thereby, it also seems that game type and LE are potential variables that can influence metabolic responses to AVG6, 13,14,15.
Physical inactivity increases the risk of cardiovascular diseases such as diabetes and its comorbidities, such as metabolic changes related to hormones and glycemic control2. Although PA is one of the principal therapies recommended for people with diabetes2, it is not known if people with diabetes can use AVG safely. Some elevation in risk can occur with increased PA, and specific precautions need to be made to lower these risks, mainly if these persons are unaccustomed to exercise17. Thus, requirements for evidence-based medicine have indicated that each tool used in the therapeutic process should be assessed for safety in healthy volunteers before diabetics18.
The rationale of this study relies upon the fact that effective BG and blood pressure control prevents cardiovascular events and that AVG effects are still unclear as to type, duration, and intensity. This study aimed to analyze acute glycemic and cardiovascular responses of a 30-minute AVG session at moderate-intensity in healthy adults (before in diabetics) and their LE after the game. We hypothesized that an AVG session at a moderate- intensity promotes acute BG and blood pressure reduction post-session, increasing cardiovascular variables at safe levels, as well as high LE during the practice. The present investigation has the potential to elucidate the effects of AVG in relation to glycemic levels and post-exercise hypotension.
Participants were recruited from a university campus via word of mouth advertising and social media websites. All study participants (n= 14) were fully informed about the protocol and procedures and provided written informed consent, as approved by the local ethics committee for human research (nº 029770/16). Inclusion criteria were: university students, 19≤aged≤44 years, being healthy (non-diabetic or hypertensive), and physically active (≥ three moderate or vigorous physical activity days per week). Exclusion criteria were: disorders limiting the use of AVG (e.g., neurological disorders, physical, visual or cognitive impairment, deafness, vertigo), or specific medical restrictions (e.g., severe pain, preventing prescription of self-regulated training). Twelve participants reported having played Xbox Kinect before participating in the study. In order to detect a mean (standard deviation) reduction of 15 (16) mg·dL−1 in BG based on pilot study, a priori sample size calculation was estimated by G*Power 3.1.9 software (Franz Faul, University Kiel, Germany), given α= 0.05, power (1−β)= 0.8, and effect size (ES)= 0.9 (large). Thus, a minimum of 12 participants was required.
In a one-group pretest-posttest experimental design, participants underwent anthropometric, cardiovascular, and glycemic measures, and they performed a 30-minute AVG session supervised at the Human Performance Laboratory (Temperature: 22-26 ºC, Ambient relative humidity: 40-60%, Atmospheric pressure: ≈101.3 Pa). A self-report health-screening questionnaire before participation was required. All the participants familiarized themselves with the AVG for three minutes of gaming (with some information given by a physical trainer) about 1-2 minutes before data collection, but this familiarization was not included in the data analysis. Primary (blood glucose) and secondary (heart rate, systolic and diastolic blood pressure, double product) outcome measures were recorded at rest (PRE), immediately after AVG session (POST-0) and at 30 minutes after AVG (POST-30) with passive recovery in the sitting position. At the end AVG session, participants reported LE and rating of perceived exertion (RPE). Figure 1 illustrates the study design.
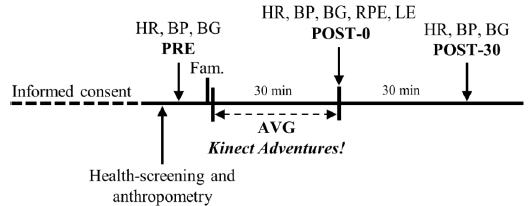
Figure 1
Study design. Heart rate (HP), blood pressure (BP) and blood glucose (BG) measurements at rest (PRE), immediately after (POST-0) and 30 minutes after (POST-30) an active video games (AVG) session. Fam., Familiarization. Rating of perceived exertion (RPE) and level of enjoyment (LE) were only measured immediately after the AVG session.
A single experienced physical trainer controlled all the sessions in order to provide standardized instructions on how to perform the game. Participants were encouraged to do their best in the AVG session, but no feedback was given during the assessment. All participants were instructed to wear minimal clothing and appropriate footwear for PA, to avoid moderate or vigorous exercise for 24 hours before testing, to feed 1-2 hours before the assessment, and to refrain from ingesting beverages containing caffeine, others substance stimulants or alcohol during the 24 hours preceding the tests.
Anthropometry: Height (m) and body mass (kg) were recorded using a wall-mounted stadiometer (Wiso, Brazil) and a digital scale (Mic 300, Filizola, Brazil) to the nearest 0.01 m and 0.1 kg, respectively, by a single evaluator with standard techniques19. Height and body mass were used to calculate the body mass index (BMI), reported as kilograms per square meter.
Cardiovascular: During gameplay sessions, HR (bpm) was continuously monitored using an HR monitor (Polar FT4; Polar Electro, Finland). Systolic (SBP, mm Hg) and diastolic (DBP, mm Hg) blood pressure were measured on the left arm using blood pressure monitor (Omron HEM 7113; Omron Healthcare Co. Ltd., Japan). All cardiovascular measures were taken in the sitting position, and the participants were asked to remain without speaking or moving. Double product (DP) was calculated as SBP × HR (mm Hg × bpm) for the same period, providing valuable information on the cardiac workload and myocardial oxygen demand. Average, maximal, and percent HR reserve were calculated according to a prior study7 and used for characterizing the session intensity.
Capillary blood glucose: Capillary blood samples (at fingertips) were collected using standard procedures20. BG (mg·dL−1) was assessed using a clinical glucometer (Accu-Check Active, Roche, Brazil), that assessed glycemic levels in approximately five seconds, and a lancet device, disposable test strips, and disposable lancets (Accu-Check Softclix, Roche, Brazil).
Level of enjoyment: A 100-mm Visual Analog Scale (VAS)21 in the paper-and-pencil form, ranging from 0 (very boring) to 100 (very enjoyable), was used to measure LE22 immediately after the session.
Rating of perceived exertion: RPE was self-reported on a scale of 6-20 (Borg Scale)23, which is frequently used to assess the level of exercise intensity as muscular subjectively, cardiovascular (tachycardia/bradycardia) and respiratory (hyperventilation) effort. Perceived exertion was defined as “How tired did your body feel while you were playing AVG, analyzing your perception of cardiorespiratory and skeletal muscles?”.
AVG sessions were performed using an Xbox 360 Kinect game console (Microsoft, USA). A multimedia projector (Power lite S10+, Epson, Japan) with a sound amplifier (OCM 126 professional, Oneal, Brazil) was used as an AVG device. The setup lab measurement was described previously7, 8. Kinect Adventures! game (Microsoft Game Studios, USA) was chosen for the use of large muscle groups, attending recommendations for PA programs, which should include appropriate endurance exercise for developing and maintaining cardiorespiratory fitness, body composition, and muscular strength and endurance2. In addition, this game provides low risk to the osteomyoarticular health of its practitioners24. In a previous analysis, participants reached a moderate-intensity in almost all mini-games of “Kinect Adventures!” game. Moreover, it is an AVG that is part of the console when it is bought.
In this study, participants played 10 minutes of the three most intense mini-games, respectively: River Rush, Rally Ball, and Reflex Ridge. River Rush game targets to gather as many pins as are in the water/air. In the Rally Ball game, participant deflects balls and hit them down the court, and at the same time collecting the balls (preventing them passing). Reflex Ridge game aims to race on a platform, jump over hurdles, lean away from obstacles, and limbo to avoid hitting their heads on low beams25. In all mini-games, participants performed jumps, squats, and lateral shifts with vertical and horizontal shoulder extension (or combining them) collecting all possible pins.
Outcome measures presented normal distribution (Shapiro-Francia test), except HR. When the normality assumption was accepted, the data were presented as mean and standard deviation (SD). Otherwise, data were reported by median and interquartile range. Independent t-test or Mann-Whitney test did not indicate baseline differences between sexes for outcome measures. Therefore, repeated-measures one-way analysis of variance grouping men and women together compared the PRE, POST-0, and POST-30 values. Mauchly's test was used to test the assumption of sphericity, and when it was violated, technical corrections were performed using the Greenhouse-Geisser test. When significant differences were detected, Bonferroni pairwise comparisons were performed. Friedman's test adjusted by the Bonferroni correction for multiple tests was applied to compare the HR values over time. Percent changes in outcome variables were calculated (%∆= [(POST-0 or POST-30 − PRE)/PRE] × 100). Effect size (ES) was calculated using Cohen’s d statistic26, which an ES of d= 0.01-0.20 was considered small, d= 0.21-0.50 moderate, d= 0.51-0.80 large, and d≥ 0.80 very large27. Besides, two-way mixed model intraclass correlation coefficient (ICC3,1) and standard error of measurement (SEM= SDpool × √1 − ICC) were calculated to estimate the minimum detectable difference (MDD) for glycemic values (PRE/POST-0) as follows: MDD= SEM × 1.96 × √2 (95% confidence interval). The level of significance was set at P<0.05 (α= 0.05). The IBM SPSS Statistics 24.0 (IBM SPSS Inc., USA) was used.
Fourteen healthy adults, seven males [Mean (SD), age: 24 (6) years, mass: 69.3 (5) kg, height: 1.72 (0.03) m, body mass index: 23.3 (1.2) kg·m−²] and seven females [Mean (SD), age: 22 (4) years, mass: 59.3 (3) kg, height: 1.63 (0.02) m, body mass index: 22.4 (1.0) kg·m−²] participated in this study. Most of the participants reported a family history of diabetes (71.4%). They performed exergames at an intensity of 55.5% (SD= 8.5) HR reserve. Maximal and average HR were 169 bpm (SD= 21) and 130 bpm (SD= 18), respectively. LE and RPE were 8.6 (SD= 1.1) and 15 (SD= 2) at the end of the session, respectively.
Table 1 shows acute BG, SBP, DBP, and DP responses over time. BG changed over time (F1.4, 18.4= 5.1, P= 0.025). There was a statistical reduction in BG at POST-0 in comparison to the PRE (%Δ= −9.1, P= 0.001, d= 0.94). MDD for BG was equal to 15.1 mg·dL−1.
Glycemic and cardiovascular responses of healthy adults at rest (PRE), immediately after (POST-0) and at 30 minutes after (POST-30) a 30-minute AVG session (n= 14)
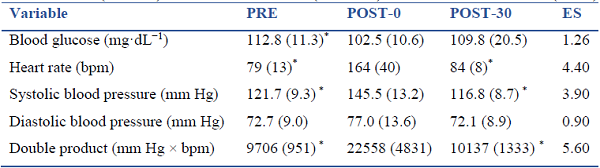
Data reported by mean (SD), except heart rate expressed by median (interquartile range).
* Significant difference to the POST- 0 (P<0.05). ES, effect size (ANOVA main effect).A time effect was detected for HR (χ22= 23.3, P= 0.001), SBP (F1.3, 16.6= 49.6, P= 0.001) and DP (F1.1, 14.6= 107.6, P= 0.001). No differences were found in DBP (F2, 26= 3.1, P= 0.062). There was a statistical increase in HR at POST-0 in comparison to the PRE values (%Δ= +107.6, P= 0.001). SBP at POST-0 was statistically greater than at PRE (%Δ= +19.7, P= 0.001). There was a slight hypotension effect (non-statistical) in SBP at POST-30 (%Δ= −4.3, P= 0.116). DP at POST-0 was statistically greater than at PRE (%Δ= +132.4, P= 0.001).
This study analyzed acute glycemic and cardiovascular responses of 30-minute continuous AVG session with “Kinetic Adventures!” game in non-diabetic adults and yours LE after the game. Our findings confirmed partially the hypothesis an AVG session at moderate- intensity promotes BG reduction and cardiovascular increase (HR, SBP, and DP), as well as high LE, while DBP was unaltered. Previous studies with AVG have examined HR and/or blood pressure in several settings7,8,9, 11, 14, 16. However, this was the first investigation to explore BG responses while playing AVG commensurate with the moderate (by HR reserve) or vigorous (by RPE) intensity according to ACSM1. This fact reinforces the need for using both subjective and objective measures when assessing neurophysiological responses6.
Although MDD for BG was about 15 mg·dL−1, glycemic levels reduced about 10 mg·dL−1 (large ES) immediately after the AVG session. This ES indicates 82% of the values at POST-0 will be above the mean of the PRE moment, and there is a 74% chance that a person picked at random from the POST-0 will have a higher score than a person picked at random from the PRE moment (probability of superiority)28. It is known that an acute bout of exercise induces an insulin-independent translocation of glucose transporter type 4 (GLUT-4) to the cell surface and increases insulin-stimulated whole-body glucose uptake12. Thus, as with other forms of aerobic exercise, AVG at a moderate-intensity can act with synergistic action with insulin in insulin-sensitive tissues2, although effect duration at POST-30 was not detected.
Soltani and Salesi11 observed the combination of music and an AVG (Wii Fit Running) as a video intervention have a significant change in the total time of running, however, they did not find any statistical effect on changing levels of BG compared with the control or other training groups. Our findings did not corroborate with these results, probably because their intervention intensity may have been light due to the use of Nintendo Wii, in which participants may underestimate body movements from the fact of his motion sensor is an accelerometer24, using for example just the hands and wrists. Also, the longest Wii Fit Running session lasted only about 18 minutes11. Thereby, BG reductions related to AVG sessions seem to depend on intensity and duration.
In general, there is a dose-dependent effect of intensity and duration on the cardiovascular changes following aerobic exercise29. Our AVG session resulted in greater values immediately after the session, and, despite the nonsignificance, SBP presented the expected hypotensive effect after 30 minutes of passive recovery, while DBP showed an even slighter reduction. Once HR at the POST-30 was slightly higher than PRE values, it seems cardiac output remained high and, therefore, systolic hypotension was limited. Moreover, participants presented high levels of LE, which may have provided a greater release of catecholamines6 and hence influenced the HR at POST-30.
DP values at POST-0 suggest the AVG session induced substantial stress on the heart with lower blood pressure overload. Thus, cardiac workload and myocardial oxygen demand were similar to an aerobic exercise bout. Such as exercise capacity (in metabolic equivalents - METs) for example, DP is an essential feature of exercise, and it can be measured as a useful hemodynamic predictor for cardiovascular mortality (DP reserve) and when evaluating the efficacy of therapy30. Similarly to our findings, Neves et al.16 showed an increase of about 97% on the DP of healthy adults after a 22-minute Zumba Fitness Core® game session. Nonetheless, further research should be conducted to investigate other cardiovascular changes for AVG at different intensities and durations.
Kinetic Adventures! game yielded LE levels closer to 100% “Very Enjoyable” by VAS. Mellecker et al.6 highlight this game inspires triumphant affective expressions by offering opportunities to make one's trophies by striking a pose upon concluding a level. Therefore, these embodiment characteristics may contribute to feelings of fun during play and induce similar physiological effects to those of classical PA with the experience of enjoyment6. These results were analogous to other studies with young adults such as the analyses of two different AVG (Kinect Sports Boxing and Nike Kinect Fitness), which showed high LE levels over 6- week training7 and another research with six different AVG found they were more enjoyable than traditional exercise (cycling)13.
Our data, obtained from healthy adults, demonstrate the relevant role of AVG to promote beneficial and safe cardiovascular changes by a very enjoyable form of exercise. Moreover, this study provides the first reference for acute reduction of BG in healthy individuals by AVG. High levels of sedentary behavior such as screen time may be partially modified using AVG, once Kinect Adventures! game session met the current recommendations for PA3. In addition, enjoyment exercise by AVG can remain high over the weeks, supporting the process of individual behavior change7. Thus, our findings have practical applications for improving PA from attractive exercise forms, and it seems reasonable to recommend that people with diabetes can use this form of PA10,11. Even though AVG sessions can be performed at home, the authors genuinely recommend a professional prescription once there is AVG with numerous objectives8.
Although the participants were normoglycemic, a control session (passive rest/recovery) could better evidence of the individual BG control compared to AVG at the moderate/vigorous intensity. In our investigation, the sample size was restricted to detect only statistically large ES (d≥ 0.9), this could be a limitation of the study. It is known that minor cardiometabolic changes elicited by PA, such as blood pressure reduction, bring potential health benefits, especially for special populations (e.g., hypertensive or diabetic patients). Nevertheless, we calculated a priori power for BG as the primary outcome. Another limitation was that the participants' range of motion during gameplay was not evaluated, and although standardized instructions have been given, there was undoubtedly variation in exact movement among participants, which can affect physiological responses.
A 30-minute AVG session (Kinetic Adventures! game) at moderate-intensity was considered very enjoyable and effective in reducing blood glucose levels and promote safe cardiovascular acute changes in healthy adults.
Cite it like this:: Brito-Gomes JL, Oliveira, LS,Vancea DMM, Costa MC. Do 30 minutes of active video games at a moderate-intensity promote glycemic and cardiovascular changes?
Disclosure statement: No competing financial interests exist.
Universidade Federal do Vale do São Francisco, Centro, Petrolina, Pernambuco, Brazil. Zip code: 56304917 jorgelbritog@hotmail.com
Figure 1
Study design. Heart rate (HP), blood pressure (BP) and blood glucose (BG) measurements at rest (PRE), immediately after (POST-0) and 30 minutes after (POST-30) an active video games (AVG) session. Fam., Familiarization. Rating of perceived exertion (RPE) and level of enjoyment (LE) were only measured immediately after the AVG session.
Glycemic and cardiovascular responses of healthy adults at rest (PRE), immediately after (POST-0) and at 30 minutes after (POST-30) a 30-minute AVG session (n= 14)
Data reported by mean (SD), except heart rate expressed by median (interquartile range).
* Significant difference to the POST- 0 (P<0.05). ES, effect size (ANOVA main effect).